Minute Distance.
The minute distance is how far the red blood cells travel in one minute, which might seem a strange thing to want to know until you realise that this is the mean flow rate in the aorta (or pulmonary artery). Just picture a river flowing. If the river is silting up or obstructed by fallen trees or abandoned cars, then the river flows slowly or almost stagnates. A healthy river without obstruction flows swiftly. The flow rate tells us how patent the peripheral circulation is, and also how easily the blood can flow through it which, as mentioned above, depends to a large extent on viscosity. Just picture the same river, but instead of water it was mud flowing. How fast would the flow be then?
The normal flow rate for the aorta (aortic minute distance or AMD) is 14-22 m/min (10-16 m/min for the pulmonary artery, PMD.). Suddenly the concept of hyperdynamic and hypodynamic circulation becomes clear. An aortic flow rate of 10 m/min is too slow, it is hypodynamic. An AMD of 28 m/min on the other hand is too fast and represents a clearly hyperdynamic circulation.
So now we know how to optimise preload, gauge myocardial contractility, and judge afterload, and we can measure stroke volume and cardiac output. Along with the blood pressure, we now have all the tools we need to optimise hemodynamics in the hypotensive patient.
Take a look at the figures below generated by the USCOM for a 30 year old 60Kg female with a BP of 70/40. What is your diagnosis?
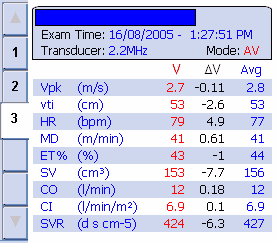
If we scan down the values for Vpk, heart rate, MD, SV, CO, CI and SVR then it is obvious we are dealing with a powerfully contracting heart which is generating a hyperdynamic circulation (AMD = 41 m/min) with an SV of around 2.5mls/kg, about double the value we would normally expect. This is generating a high CO of 12 L/min with a cardiac index of 6.9 L/min/m2. Clearly the hypotension is not due to a failing myocardium! The answer is immediately apparent when we look at SVR, it is just about one third of normal. We are looking at marked peripheral vasodilation, vascular collapse if you like. This is a high-output, hyperdynamic state as a result of septicaemia. The heart is working almost maximally to increase the CO to try to raise the BP, but with an SVR this low, the heart just can’t generate enough CO to compensate. The treatment? Raise the SVR to a value closer to 1200, and you know how to do that from what’s gone before. Easy as painting by numbers!
But the USCOM isn't just about acute medical conditions. What about hypertension and chronic heart failure? Can the USCOM guide our therapy here? You bet it can!
|

